


 Sign Out
Sign Out
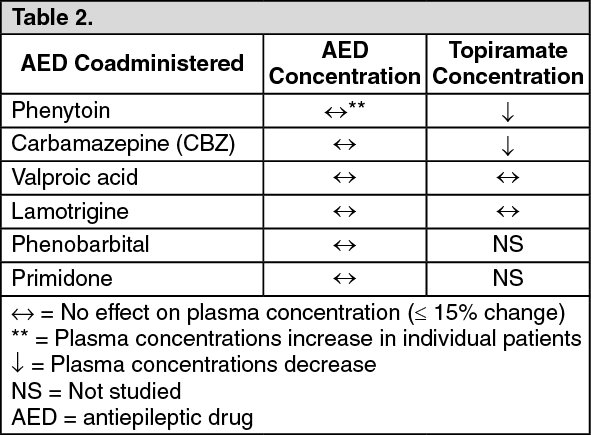
A pharmacokinetic interaction study of patients with epilepsy indicated the addition of topiramate to lamotrigine had no effect on steady state plasma concentration of lamotrigine at topiramate doses of 100 to 400 mg/day. In addition, there was no change in steady state plasma concentration of topiramate during or after removal of lamotrigine treatment (mean dose of 327 mg/day).
Topiramate inhibits the enzyme CYP 2C19 and may interfere with other substances metabolized via this enzyme (e.g., diazepam, imipramin, moclobemide, proguanil, omeprazol).
Effects of other antiepileptic medicinal products on topiramate: Phenytoin and carbamazepine decrease the plasma concentration of topiramate. The addition or withdrawal of phenytoin or carbamazepine to topiramate therapy may require an adjustment in dosage of the latter. This should be done by titrating to clinical effect. The addition or withdrawal of valproic acid does not produce clinically significant changes in plasma concentrations of topiramate and, therefore, does not warrant dosage adjustment of topiramate. The results of these interactions are summarized as follows: (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOther medicinal product interactions: Digoxin: In a single-dose study, serum digoxin area under plasma concentration curve (AUC) decreased 12% due to concomitant administration of topiramate. The clinical relevance of this observation has not been established. When topiramate is added or withdrawn in patients on digoxin therapy, careful attention should be given to the routine monitoring of serum digoxin.
CNS depressants: Concomitant administration of topiramate and alcohol or other CNS depressant medicinal products has not been evaluated in clinical studies. It is recommended that topiramate not be used concomitantly with alcohol or other CNS depressant medicinal products.
St John's Wort (Hypericum perforatum): A risk of decreased plasma concentrations resulting in a loss of efficacy could be observed with co-administration of topiramate and St John's Wort. There have been no clinical studies evaluating this potential interaction.
Oral contraceptives: In a pharmacokinetic interaction study in healthy volunteers with a concomitantly administered combination oral contraceptive product containing 1 mg norethindrone (NET) plus 35 μg ethinyl estradiol (EE), topiramate given in the absence of other medications at doses of 50 to 200 mg/day was not associated with statistically significant changes in mean exposure (AUC) to either component of the oral contraceptive. In another study, exposure to EE was statistically significantly decreased at doses of 200, 400, and 800 mg/day (18%, 21%, and 30%, respectively) when given as adjunctive therapy in epilepsy patients taking valproic acid. In both studies, topiramate (50-200 mg/day in healthy volunteers and 200-800 mg/day in epilepsy patients) did not significantly affect exposure to NET. Although there was a dose dependent decrease in EE exposure for doses between 200-800 mg/day (in epilepsy patients), there was no significant dose dependent change in EE exposure for doses of 50-200 mg/day (in healthy volunteers). The clinical significance of the changes observed is not known. The possibility of decreased contraceptive efficacy and increased breakthrough bleeding should be considered in patients taking combination oral contraceptive products with topiramate. Patients taking estrogen containing contraceptives should be asked to report any change in their bleeding patterns. Contraceptive efficacy can be decreased even in the absence of breakthrough bleeding.
Lithium: In healthy volunteers, there was an observed reduction (18% for AUC) in systemic exposure for lithium during concomitant administration with topiramate 200 mg/day. In patients with bipolar disorder, the pharmacokinetics of lithium were unaffected during treatment with topiramate at doses of 200 mg/day; however, there was an observed increase in systemic exposure (26% for AUC) following topiramate doses of up to 600 mg/day. Lithium levels should be monitored when co-administered with topiramate.
Risperidone: Drug-drug interaction studies conducted under single dose conditions in healthy volunteers and multiple dose conditions in patients with bipolar disorder, yielded similar results. When administered concomitantly with topiramate at escalating doses of 100, 250 and 400 mg/day there was a reduction in risperidone (administered at doses ranging from 1 to 6 mg/day) systemic exposure (16% and 33% for steady-state AUC at the 250 and 400 mg/day doses, respectively). However, differences in AUC for the total active moiety between treatment with risperidone alone and combination treatment with topiramate were not statistically significant. Minimal alterations in the pharmacokinetics of the total active moiety (risperidone plus 9-hydroxyrisperidone) and no alterations for 9-hydroxyrisperidone were observed. There were no significant changes in the systemic exposure of the risperidone total active moiety or of topiramate. When topiramate was added to existing risperidone (1-6 mg/day) treatment, adverse events were reported more frequently than prior to topiramate (250-400 mg/day) introduction (90% and 54% respectively). The most frequently reported AE's when topiramate was added to risperidone treatment were: somnolence (27% and 12%), paraesthesia (22% and 0%) and nausea (18% and 9% respectively).
Hydrochlorothiazide (HCTZ): A drug-drug interaction study conducted in healthy volunteers evaluated the steady-state pharmacokinetics of HCTZ (25 mg q24h) and topiramate (96 mg q12h) when administered alone and concomitantly. The results of this study indicate that topiramate Cmax increased by 27% and AUC increased by 29% when HCTZ was added to topiramate. The clinical significance of this change is unknown. The addition of HCTZ to topiramate therapy may require an adjustment of the topiramate dose. The steady-state pharmacokinetics of HCTZ were not significantly influenced by the concomitant administration of topiramate. Clinical laboratory results indicated decreases in serum potassium after topiramate or HCTZ administration, which were greater when HCTZ and topiramate were administered in combination.
Metformin: A drug-drug interaction study conducted in healthy volunteers evaluated the steady-state pharmacokinetics of metformin and topiramate in plasma when metformin was given alone and when metformin and topiramate were given simultaneously. The results of this study indicated that metformin mean Cmax and mean AUC0-12h increased by 18% and 25%, respectively, while mean CL/F decreased 20% when metformin was co-administered with topiramate. Topiramate did not affect metformin tmax. The clinical significance of the effect of topiramate on metformin pharmacokinetics is unclear. Oral plasma clearance of topiramate appears to be reduced when administered with metformin. The extent of change in the clearance is unknown. The clinical significance of the effect of metformin on topiramate pharmacokinetics is unclear.
When topiramate is added or withdrawn in patients on metformin therapy, careful attention should be given to the routine monitoring for adequate control of their diabetic disease state.
Pioglitazone: A drug-drug interaction study conducted in healthy volunteers evaluated the steady-state pharmacokinetics of topiramate and pioglitazone when administered alone and concomitantly. A 15% decrease in the AUCƮ,ss of pioglitazone with no alteration in Cmax,ss was observed. This finding was not statistically significant. In addition, a 13% and 16% decrease in Cmax,ss and AUCƮ,ss respectively, of the active hydroxy-metabolite was noted as well as a 60% decrease in Cmax,ss and AUCƮ,ss of the active keto-metabolite. The clinical significance of these findings is not known. When topiramate is added to pioglitazone therapy or pioglitazone is added to topiramate therapy, careful attention should be given to the routine monitoring of patients for adequate control of their diabetic disease state.
Glyburide: A drug-drug interaction study conducted in patients with type 2 diabetes evaluated the steady-state pharmacokinetics of glyburide (5 mg/day) alone and concomitantly with topiramate (150 mg/day). There was a 25% reduction in glyburide AUC24 during topiramate administration. Systemic exposure of the active metabolites, 4-trans-hydroxy-glyburide (M1) and 3-cis-hydroxyglyburide (M2), were also reduced by 13% and 15%, respectively. The steady-state pharmacokinetics of topiramate were unaffected by concomitant administration of glyburide.
When topiramate is added to glyburide therapy or glyburide is added to topiramate therapy, careful attention should be given to the routine monitoring of patients for adequate control of their diabetic disease state.
Other forms of interactions: Agents predisposing to nephrolithiasis: Topiramate, when used concomitantly with other agents predisposing to nephrolithiasis, may increase the risk of nephrolithiasis. While using topiramate, agents like these should be avoided since they may create a physiological environment that increases the risk of renal stone formation.
Valproic acid: Concomitant administration of topiramate and valproic acid has been associated with hyperammonemia with or without encephalopathy in patients who have tolerated either medicinal product alone. In most cases, symptoms and signs abated with discontinuation of either medicinal product. This adverse reaction is not due to a pharmacokinetic interaction. An association of hyperammonemia with topiramate monotherapy or concomitant treatment with other anti-epileptics has not been established.
Hypothermia, defined as an unintentional drop in body core temperature to <35°C, has been reported in association with concomitant use of topiramate and valproic acid (VPA) both in conjunction with hyperammonemia and in the absence of hyperammonemia. This adverse event in patients using concomitantly topiramate and valproate can occur after starting topiramate treatment or after increasing the daily dose of topiramate.
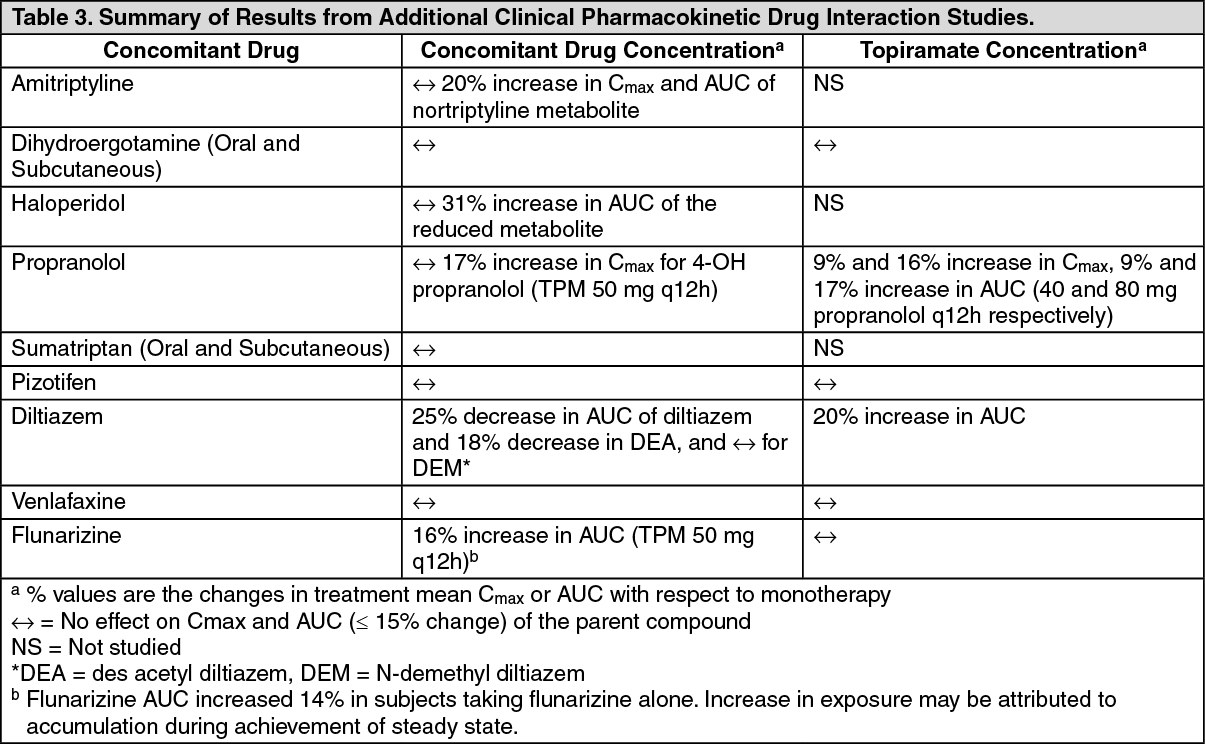
Additional pharmacokinetic drug interaction studies: Clinical studies have been conducted to assess the potential pharmacokinetic drug interaction between topiramate and other agents. The changes in Cmax or AUC as a result of the interactions are summarized as follows. The second column (concomitant drug concentration) describes what happens to the concentration of the concomitant drug listed in the first column when topiramate is added. The third column (topiramate concentration) describes how the coadministration of a drug listed in the first column modifies the concentration of topiramate. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image